Whipworm Infection in Dogs and Cats
This worm is one of the “big four” intestinal parasites with which our canine friends must often contend: roundworms, tapeworms, hookworms, and whipworms. The whipworm that affects dogs (Trichuris vulpis) is substantially smaller than the other worms (a mere 30-50 mm in length, about two inches maximum) and is rarely seen as it lives in the cecum (the part of the large intestine where the small and large intestine meet). The head (or, more accurately, the digestive end of the worm) is skinny versus its stout tail (or reproductive end), which gives the worm a whip shape, hence the name.
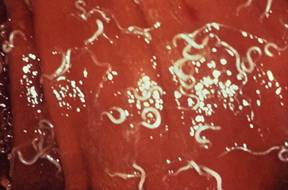
In the host’s digestive tract, food passes from the mouth to the esophagus to the stomach to the small intestine to the large intestine to the rectum, and then to the outside world. This means the large intestine is one of the last stops for nutrients, and by this point in the journey, nutrients have largely been broken down and absorbed. The large intestine is the home of the whipworm. The adult worms bite the tissue of the intestine, actually embedding their heads inside, and suck blood there.
Eggs are laid inside the large intestine and pass with the stool. Once in the outside world, the eggs require about two-to-four weeks to form embryos and become capable of infecting a new host. (This means that contaminated soil is the source of infection, not fresh feces.)
The new host is infected by consuming the egg, usually during grooming. After the host eats it, the egg hatches in the host’s small intestine releasing a larva.
The larva dives into the local glandular tissue and, after about a week, emerges into the small intestine and is carried downstream into the large intestine with the digested food. Once in the cecum or large intestine, its permanent home, it embeds in the tissue there, and after a total of 74 to 87 days from the time the egg was swallowed, the young whipworm is ready to mate.
Signs of Infection
A few whipworms generally do not pose a problem for the host, but if large numbers of worms are embedding themselves in the large intestine tissue, tremendous inflammation can result, leading to bloody, gooey diarrhea. Usually, there is not enough blood loss to be dangerous, but diarrhea readily becomes chronic and hard to control. A second syndrome of infection has emerged but is not well understood: signs mimicking those of Addison’s disease (hypoadrenocorticism). Here, waxing and waning weakness with the inability to conserve salt ultimately creates a dehydration crisis. The syndrome mimics Addison’s disease in every way except that testing for Addison’s disease will be negative and deworming yields a complete recovery.
Because female whipworms only periodically lay eggs (whereas other female worms lay eggs continuously), a fecal sample tested may easily be negative for eggs. This makes confirmation of a whipworm infection a challenge. It is common to deworm whipworms if the symptoms are suggestive of their presence, even if the fecal test is negative. Most common deworming agents do not work on whipworms, so something special must be selected. The most common products are fenbendazole (Panacur®), and febantel (Drontal Plus®).
Thanks to the long maturation cycle of young worms, a second deworming some 75 days or so after the first deworming is needed to fully clear the infection (easy to forget). Often another deworming in between these doses is recommended to further control the whipworm numbers.
Products Effective against Whipworms
More recently, regular heartworm prevention products have been developed to remove and control whipworms: Milbemycin-based heartworm preventives (such as Sentinel®, Interceptor®, and Trifexis®) will cover whipworms, and their regular use covers the second deworming as well. Moxidectin based heartworm preventive, such as Advantage Multi® and similar products, will also cover whipworms.
Soil contaminated by whipworm eggs is contaminated for years. It is virtually impossible to remove the eggs from the soil or kill them. This potential for environmental contamination is concerning, but while there are scattered reports in the medical literature supporting human infection, the Companion Animal Parasite Council does not consider the canine whipworm to be transmissible to humans until there is stronger evidence.
Feline Whipworm Infection

There are species of whipworms that can infect cats: Trichuris serrata in North America and Trichuris campanula in Europe. Cats are clean animals and fastidious around feces, and they rarely get infected. When they do, worm numbers are so small that symptoms hardly ever occur. Whipworms are more of an interesting incidental finding in cats when whipworm eggs happen to come up on a routine fecal check. In other words, feline whipworm infection is generally not considered to be much of a problem.












